Healthcare App Marketing: Growth Strategies for Telemedicine and Wellness Apps
Healthcare app marketing is constrained by privacy, regulation, and a higher trust bar than any other consumer vertical. Here is the playbook that works.

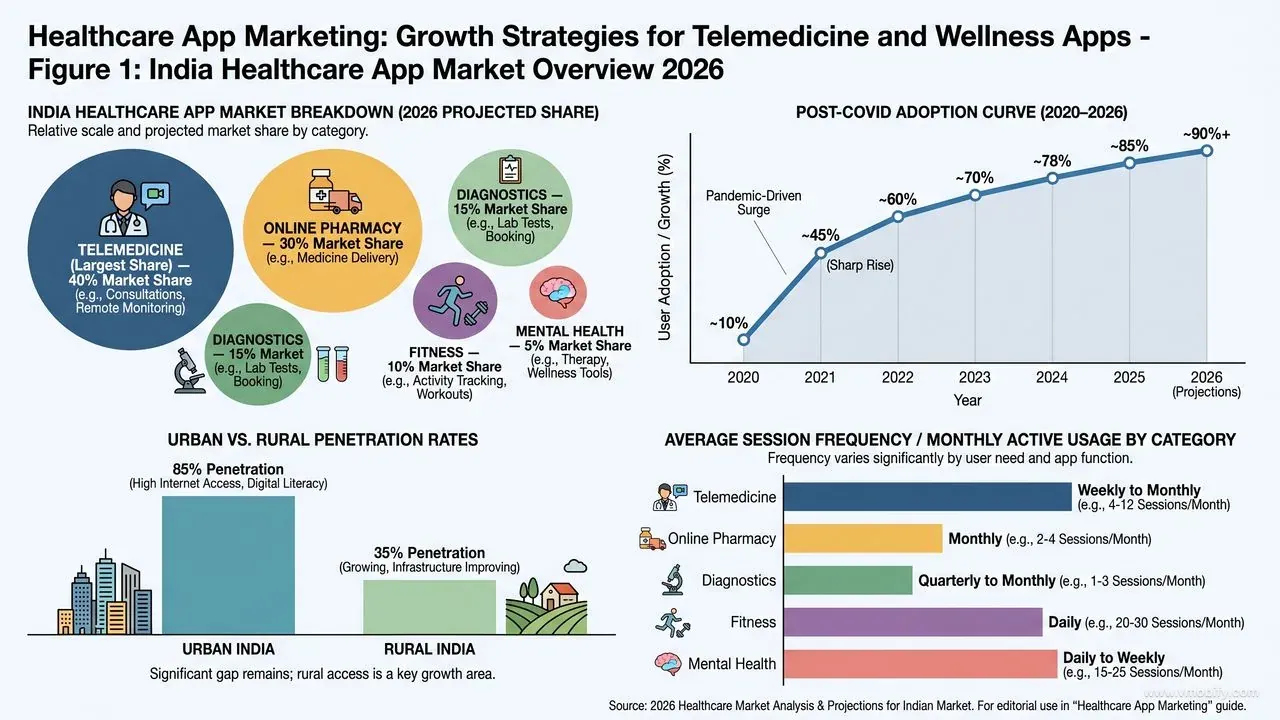
What does the Indian healthcare app market look like in 2026?
India's healthcare app market is now the second-largest in the world by monthly active users, but it is also the most compliance-constrained consumer vertical — standard performance marketing playbooks fail here on contact.
Post-COVID adoption permanently changed how Indians access care. Telemedicine consultations, online pharmacy, diagnostic bookings, fitness and wellness, and mental health apps now collectively reach several hundred million monthly users. Practo, Tata 1mg, PharmEasy, Apollo 24/7, Cult.fit, Wysa and a long tail of category-specialised apps have matured the supply side; Statista's India mobile usage data shows healthcare app penetration roughly tripled between 2020 and 2025.
But the regulatory envelope is unlike any other vertical. ASCI guidelines, the Drugs and Magic Remedies (Objectionable Advertisements) Act, MCI/NMC rules on doctor advertising, and platform-level health-category policies on Google and Meta each shape what you can say, who you can target, and how you can verify outcomes. The DPDP Act 2023 added a sharper consent and data-handling layer on top — health data is "sensitive personal data" and mishandling it carries material financial penalty.
Layer on top the consumer-side reality: medical decisions trigger a level of caution that no other vertical sees. Users research, compare, abandon, and return weeks later. A creative that drives a hyper-casual install in 8 seconds will take 3-5 sessions to drive a healthcare consult booking. AppsFlyer's State of App Marketing reports show install-to-first-purchase windows in health and wellness running 2-4x longer than in ecommerce or gaming.
Across our 300+ apps managed since 2013, the healthcare apps that win are the ones that internalise this asymmetry early — they engineer for trust accumulation, not for instant conversion. The losers run aggressive performance-marketing playbooks borrowed from D2C or gaming, hit a wall at ~15% install-to-active conversion, and burn through budget trying to fix it on the creative side when the actual fix lives in funnel architecture and credential surfacing. The teams we have seen succeed in Indian healthcare typically restructure their app's first three sessions before they restructure their ad account — and the order matters.
Which healthcare app category models matter?
Healthcare is not one market — it is six distinct categories with different CPI bands, different conversion funnels, and different retention economics. Treating "healthcare" as a single bucket is the most common strategic error we see.
- Telemedicine consult (CPI ₹60-180): ARPU varies hugely by consult type — general physician ₹250-500, specialist ₹600-1,500, mental health ₹800-2,000. Install-to-first-consult conversion 8-18%. Spend ceiling is set by doctor supply, not demand.
- Online pharmacy (CPI ₹40-110): Repeat-order economics dominate the model. First-order conversion 15-30%, but the lifetime value lives in subscription refills and chronic-care customers. The 90-day repeat rate is the only metric that matters.
- Diagnostic / lab booking (CPI ₹50-140): Conversion to first test 5-15%; basket size is the second key metric. Home-collection serviceability of the user's pincode dominates conversion — geo-targeting matters more here than in any other healthcare sub-category.
- Fitness / workout (CPI ₹25-80): Lowest CPI in healthcare because creative rules are loosest. Subscription conversion 4-12%; week-4 retention is the make-or-break metric for unit economics.
- Mental health / meditation (CPI ₹40-110): Subscription conversion 3-10%; retention is structurally harder than acquisition. Apps like Wysa and Headspace solved discovery years ago — the unsolved problem is sustaining a daily-use habit past week 6.
- Insurance + health combo (CPI ₹120-300): First-purchase value is the highest in the vertical, but trust bar is also the highest. See our insurance app marketing playbook for the regulated-product specifics.
The categories also differ on which paid channel scales best. Pharmacy and diagnostics scale on Google UAC because intent is high and searchable. Fitness scales on Meta because creative-driven discovery works. Mental health scales on Apple Search Ads (iOS-skewed audience, high willingness to pay). Telemedicine straddles all three. Mapping your category to the right primary channel before you spend is non-negotiable — our UA team typically builds this allocation model in week 1 of any healthcare engagement.
One commercial nuance worth flagging: the gap between paid CPI and blended CPI (after organic lift) is wider in healthcare than in most verticals. Healthcare apps with strong brand and partner-hospital recognition often see organic representing 40-60% of installs once the app reaches scale. That blended view is the only one that should drive paid budget decisions — judging healthcare campaigns on paid-only CPI overstates cost and understates the marginal value of brand-led creative investment.
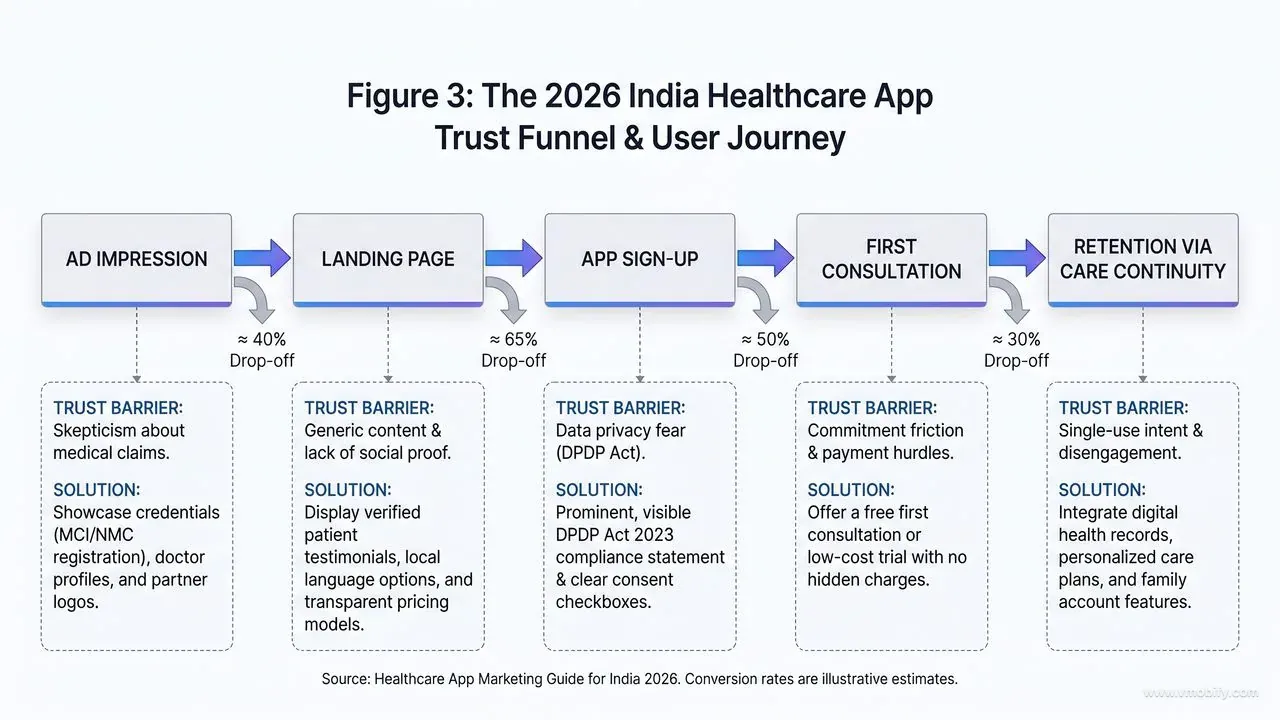
How does the trust-first funnel actually work?
In healthcare, the install is the easy part. Converting an install into a trusted, active patient requires a deliberately sequenced trust funnel — and the sequence matters more than the content of any single step.
The trap most healthcare apps fall into is treating onboarding the way ecommerce apps treat it: ask for ID, ask for permissions, push to purchase. Users in a medical context interpret that sequence as "this app wants my data before it has earned anything from me" and churn at 60-80% within the first session. The fix is reversing the order:
- First session — credibility upfront: Surface doctor credentials, certifications, partner hospitals, and short patient testimonials within the first 60 seconds. "AIIMS-trained specialists. 50,000+ consults completed. Apollo partnership" is the kind of compressed credibility statement that earns the right to ask for anything else. Generic "welcome to our app" onboarding fails the trust test before it begins.
- Frictionless first action: "Book a free symptom check" or "Get free first consult" reduces commitment friction to near-zero. The goal of session 1 is to deliver a real piece of value — a triage answer, a free first-time consult, a personalised plan — before any monetisation ask. Convert free-to-paid in session 2 or 3, never session 1.
- Identity verification timing: KYC and Aadhaar verification are eventually required for medical records and prescription handling, but never on day 1. Push verification flows after the user has experienced value — typically at the point of booking a paid consult or ordering medication. Day-1 KYC kills 30-50% of healthcare installs before they experience the product.
- Visible privacy assurance: Healthcare users worry about data leaving the app. A clear, short, plain-language data-privacy statement at signup — "Your records are encrypted. We never sell data. You can delete everything anytime." — converts materially better than the standard "I agree to the 50-page T&C" checkbox. Quote the relevant DPDP Act protection if it strengthens the assurance.
- Permission staging: Camera, location, notification, contacts — request each only when its in-context value is obvious. Notification permission asked alongside "Remind me to take my medication" converts 3-4x better than asked at app launch.
In our portfolio, healthcare apps that re-architect onboarding around this trust sequence typically lift install-to-first-consult conversion by 40-90% within the first quarter. None of it requires new product features — it requires resequencing what already exists. Pair the trust funnel with disciplined ASO on symptom and condition keywords and the same paid spend produces materially higher-quality first sessions, because the keyword that drove the install pre-loads the user with the specific intent the app then needs to serve.
What channel mix and compliance rules apply?
Healthcare creatives face stricter ad approval policies than any other consumer vertical — channel allocation has to be designed around compliance gates first and CPI economics second. The defensible mid-2026 mix for an India-focused healthcare app:
- Google UAC (40-55% of paid spend): Most healthcare-category compliant of the major platforms because you control creative and copy, and Google's healthcare-restricted product list is published and enforceable. Search Network within UAC drives the highest-intent installs — the user is already searching for a symptom or condition. Google's UAC documentation covers the bidding and creative spec; the healthcare-specific overlay sits in Google's restricted-content policy.
- Meta — health-category certified (25-35%): Requires Meta's Health Source Verification process for any medical claims or prescription-adjacent advertising. The verification adds 2-4 weeks of upfront work, but once approved, Meta delivers strong creative-driven volume — particularly for wellness, fitness, and mental health sub-categories where lifestyle creative converts. Meta's Advantage+ documentation applies, with the additional health-category creative restrictions layered on top.
- Apple Search Ads (iOS) (10-15%): High-intent, lower-volume, excellent quality. Particularly strong for wellness, meditation, and mental health apps where iOS users over-index. Apple requires a healthcare-category attestation for medical apps; once cleared, ASA is one of the cleanest channels in healthcare.
- Doctor / KOL influencer marketing (10-15%): Doctors with social presence, credentialed fitness creators, and mental health advocates deliver higher trust transfer than any paid creative possibly can. A radiologist with 80K Instagram followers explaining what shows up on a scan converts diagnostic-app installs at 3-5x the rate of polished paid creative.
- CPI / programmatic (≤10%): Use sparingly. Health-category compliance varies dramatically by network, and the retention/quality risk is higher than in other verticals. Our vetted CPI publisher set for healthcare is materially smaller than for gaming or utility — we route healthcare traffic only through publishers with explicit health-category clearance.
One critical compliance note on targeting: Meta and Google both restrict targeting based on inferred health conditions. You cannot create a Custom Audience of users who searched for "diabetes" or visited a diabetes-related URL. Healthcare campaigns rely on broad targeting plus creative-led self-selection — the creative names the condition, the user clicks if it applies, the platform never targeted them on health attributes. Violating this is one of the fastest ways to lose advertising privileges on either platform.
Which creative rules and restrictions must you follow?
Healthcare creative compliance is not a recommendation — it is a hard gate that determines whether your ads run at all. The rules are also more nuanced than most teams realise, and the highest-performing healthcare creatives sit precisely inside the compliant zone rather than near the edge of it.
- Avoid disease-cure claims absolutely: "Cures diabetes," "eliminates depression," "reverses heart disease" — all banned across every platform and likely to trigger regulator action under the Drugs and Magic Remedies Act. The compliant rephrase: "Helps manage diabetes with doctor support," "Tools for daily mental wellbeing," "Continuous heart-health monitoring." Same intent, defensible language.
- No before/after photos for medical outcomes: Especially banned for skincare, weight loss, dental, and hair-treatment apps on Meta and increasingly on Google. Lifestyle imagery, abstract progress visualisations, and verified outcome statistics (with citation) replace the before/after format.
- Credential-led creative wins: "AIIMS-trained doctors" + a real patient testimonial converts 2-3x better than benefit-led copy in our healthcare campaign data. Specificity of credential matters — "doctors" is weaker than "AIIMS-trained doctors" is weaker than "Dr. [name], 15 years at Apollo." The more verifiable the credential, the stronger the trust signal.
- Compliance-safe creative formats that work: Educational explainers ("5 signs of vitamin B12 deficiency"), service walkthroughs ("How a Practo consultation works"), reassurance-led brand creative ("Your records are encrypted and yours alone"), and credentialed-doctor explainer videos. Each of these formats has cleared both Meta and Google approval reliably in our portfolio.
- Targeting language matters: Even inside the broad-targeting requirement, the creative copy must not imply you know the user's health status. "If you have diabetes, this app helps" is acceptable. "We know you searched for diabetes — try our app" is not, even if technically you have no such targeting in place. The implication alone triggers reviewer rejection.
- Disclaimer placement: Required disclaimers ("Consult a doctor before starting any treatment", "Results may vary", "Prescription drugs sold by licensed partner pharmacies") must be readable in the creative, not buried in destination-page footer. Both platforms flag missing or unreadable disclaimers during review.
Across our healthcare portfolio, the single highest-converting creative format in 2025-2026 has been the doctor-led 30-second explainer: a real credentialed physician on camera explaining what the app does and why they recommend it to patients. It clears compliance reviews on first pass, it converts at category-leading rates, and it builds a creative library that compounds in trust over time. SplitMetrics aggregated A/B testing data shows credential-led and authority-signal creative outperforming benefit-only creative across regulated verticals consistently — and healthcare is the most regulated consumer category in the data.
One operational point most teams underweight: build a creative compliance review step into your weekly cadence. Have a clinical reviewer (a contracted physician is sufficient) sign off on the medical accuracy of every creative before it goes to platform review. Catching a compliance issue before Meta or Google does saves the 2-7 day approval delay on every iteration, and it materially reduces the risk of accumulating policy-violation strikes against the ad account.
How do you retain users via care continuity?
Healthcare retention compounds through care continuity — the more the app holds the user's medical context, the higher the switching cost. The structural levers below are what separate single-use healthcare apps from monthly-active care platforms.
- Health records integration: Allow users to upload past prescriptions, lab reports, and discharge summaries. Users with at least 3 stored records retain 5-8x better than users with none — the stored context becomes the reason they open the app for the next health event rather than starting from scratch elsewhere. ABDM (Ayushman Bharat Digital Mission) integration is now table stakes for serious Indian healthcare apps; the unified Health ID makes records portable and increases the perceived value of storing data in any single app.
- Family accounts: Multi-member profiles (parent, spouse, children, elderly parents) lift retention 3x in our portfolio and drive natural cross-category usage — a parent who books a paediatric consult often also orders the prescription and books a follow-up diagnostic. Family-account architecture is the single highest-leverage retention feature most Indian healthcare apps still under-invest in.
- Care plans and reminders: Medication reminders, follow-up consult prompts, vaccination schedules, chronic-care check-in nudges — push notifications that genuinely serve the user. The bar is whether the notification is something the user would thank you for sending. Generic engagement notifications burn permission and trigger uninstall; care-relevant notifications drive 25-40% week-on-week reactivation in our portfolio data.
- Subscription tiers (Care+ memberships): Bundle consult + pharmacy + diagnostic at a discount — Tata 1mg Plus, Apollo 24/7 Circle, PharmEasy Plus all run variants of this model. Lifts repeat-order rate, smooths revenue, and creates a switching cost beyond the records. Conversion to paid membership typically runs 3-8% of MAU in mature healthcare apps.
- Provider-side stickiness: Saved doctor relationships, ongoing therapist matching, preferred diagnostic centre — the more the app remembers about who the user trusts, the harder the app is to replace. This is the under-discussed retention lever; in mental health particularly, the therapist-match is often the entire reason a user stays.
For broader retention frameworks that apply beyond healthcare, see our app retention strategy guide. For comparable case-study results across other regulated and trust-heavy verticals, our case study portfolio documents the install-to-active funnel improvements we delivered for adjacent categories.
A final operating principle worth internalising: in healthcare, the marketing function and the clinical function cannot be separated. Every creative decision, every targeting decision, every retention nudge is also a clinical and ethical decision. Teams that treat marketing as a downstream growth function detached from the medical product consistently produce campaigns that either get rejected, get the app reviewed by regulators, or both. The healthcare apps that compound — Tata 1mg, Practo, Apollo 24/7, Cult.fit, Wysa — have all built tight feedback loops between their clinical and growth teams. The org structure shows up in the creative quality.
Talk to our healthcare team for a vertical-specific UA and retention plan calibrated to your category — telemedicine, pharmacy, diagnostic, fitness, mental health, or insurance-combo. We will map your unit economics to the channel mix, compliance pathway, and trust-funnel sequencing that fits your category and stage.
Frequently Asked Questions
Can I advertise prescription medicines on Google or Meta?+
No — direct prescription drug advertising is restricted on both platforms in India. You can advertise the platform that connects users to licensed pharmacies, with the required disclaimers visible in the creative. The product page can list prescription categories, but the ad creative cannot promote a specific Schedule H or H1 drug.
Do I need special verification to advertise a healthcare app?+
Yes on Meta (Health Source Verification, typically 2-4 weeks to clear) and increasingly on Google for healthcare-restricted products. Apple Search Ads requires a healthcare-category attestation for medical apps. Plan verification timing into your launch — campaigns cannot go live before approval clears.
What is the biggest reason healthcare apps churn?+
Single-use friction. Users install for one issue (a sore throat, a one-off lab test), get served, and never return. The structural fix is broader value — health records, family profiles, care plans, subscription bundles — surfaced before the user leaves the first session.
Are influencer doctors worth the spend?+
Usually yes. A credentialed doctor with even 50K-200K followers can convert at 3-5x the rate of paid creative for first-consult bookings, with materially higher patient quality. The compliance bar is that the doctor must be genuinely credentialed and disclose the partnership; both ASCI and MCI rules apply.
How does telemedicine CPI compare to fitness app CPI?+
Telemedicine runs 2-4x higher than fitness in India — ₹60-180 versus ₹25-80 — because regulated targeting limits audience expansion, and well-funded incumbents (Practo, Apollo 24/7, Tata 1mg) bid aggressively for category share. The LTV asymmetry justifies the higher CPI when retention works.
What is the right balance between paid UA and influencer in healthcare?+
For mid-stage apps, 70-80% paid + 10-15% influencer + 10-15% organic / ASO is a defensible mix. Influencer should index higher (20-25%) when the category is trust-heavy — mental health, paediatrics, fertility — where credentialed creators move the needle disproportionately.
How important is ASO for healthcare apps specifically?+
Very. Symptom-based search behaviour on the app stores is strong in healthcare, and our <a href="/services/aso">ASO work</a> across healthcare apps consistently lifts organic install share by 30-60% within 90 days. Symptom keywords, condition keywords, and partner-hospital brand keywords are the highest-leverage ASO targets.
Sources
- Statista — India Mobile Internet Usage — India mobile and healthcare app penetration trends 2020-2025
- Google Ads — App Campaigns Help — UAC setup, bidding, and creative best practices applicable to healthcare-restricted advertising
- Meta — Advantage+ App Campaigns Documentation — Official Meta guidance on broad targeting and Advantage+ setup, with health-category overlay
- Apple Search Ads Documentation — iOS app discovery and healthcare-category attestation requirements
- AppsFlyer State of App Marketing — Vertical-specific CPI and retention benchmarks including healthcare
- AppsFlyer Performance Index — Quarterly benchmarks for install quality and retention by category and geography
- Statista — India Influencer Marketing Market — Indian creator economy growth data underpinning doctor / KOL influencer economics
- IAMAI Reports — Industry data on India digital health adoption and regulatory context
About the author
Amol Pomane — Founder, Vmobify
Amol leads Vmobify, a mobile app growth agency that has driven 30M+ downloads and ranked 54K+ keywords across 300+ apps since 2013. He writes about ASO, paid user acquisition, retention, and the operational reality of scaling mobile apps in India and global markets.
Free Growth Audit
See exactly how to scale your app with 13+ years of expertise behind you.
Get My Strategy

